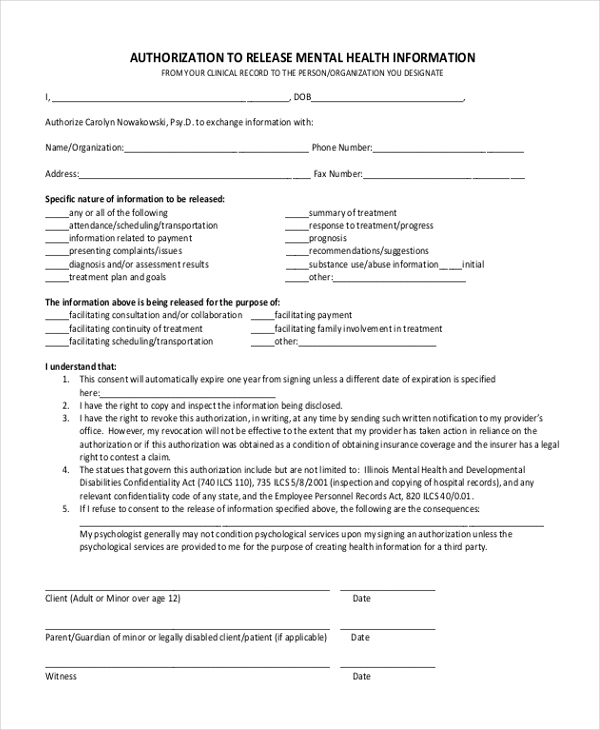
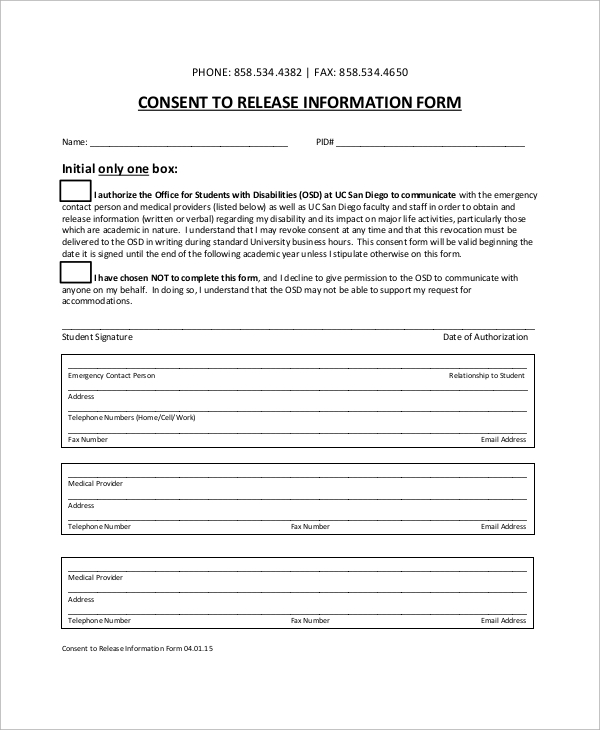
Created date 12/8/2022 10:27:22 am Ithenticate and crossref similarity check guidance is now located on a separate site. Use this form to obtain the required authorization when a request is received for patient information, unless the request received is a facsimile of this form or contains all of the required information. This form provides your therapist with written permission to communicate with other individual providers regarding your treatment (e.g. Web notice of client’s refusal to release information:
Web this template can be used to coordinate the release of confidential information during a client's transition of care or other cicrumstances where private records need to be shared. Web this template for release of information includes all of the information that you need to include and is clean, professional, easy, and fast to use. This form provides your therapist with written permission to communicate with other individual providers regarding your treatment (e.g. Web if you are a legal representative of the person whose information you are requesting, you must provide documentation proving your legal authority to the request this information (for example, power of attorney, healthcare surrogate form, order, appointment of a guardianship, order appointing Web sample standard authorization mental health treatment.
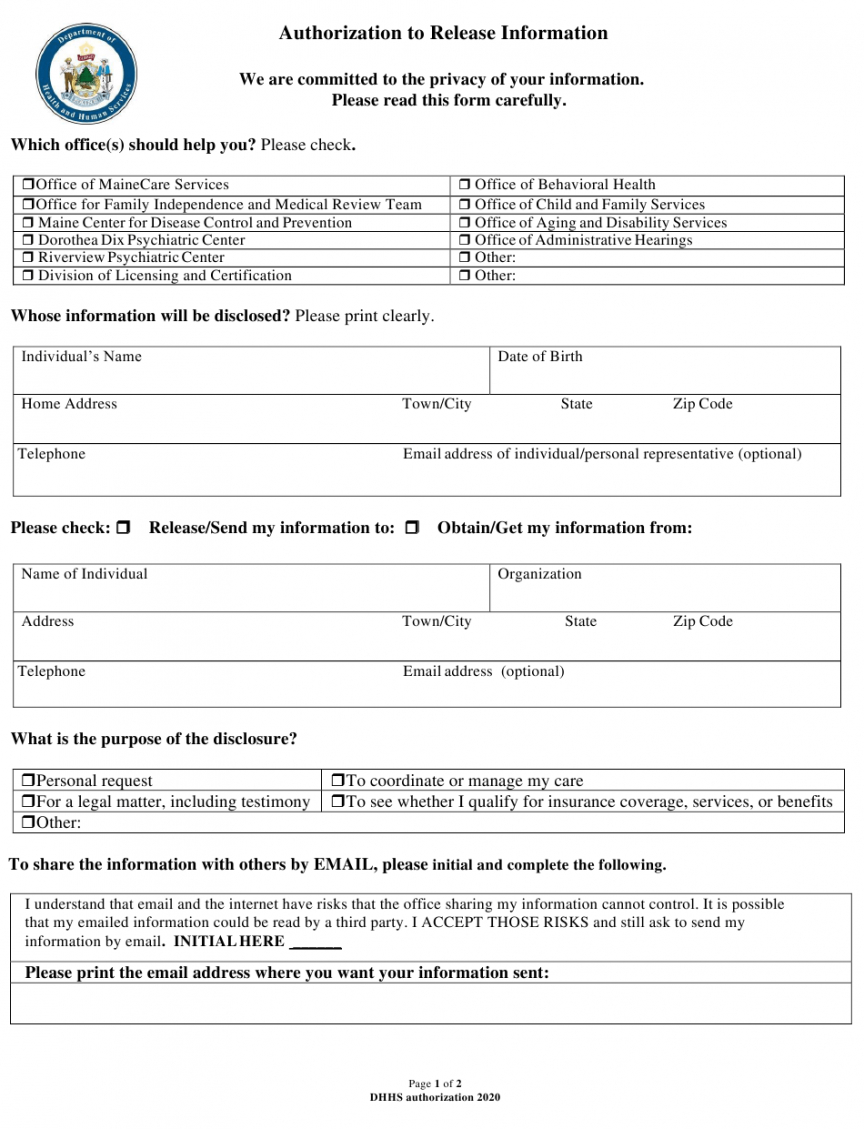
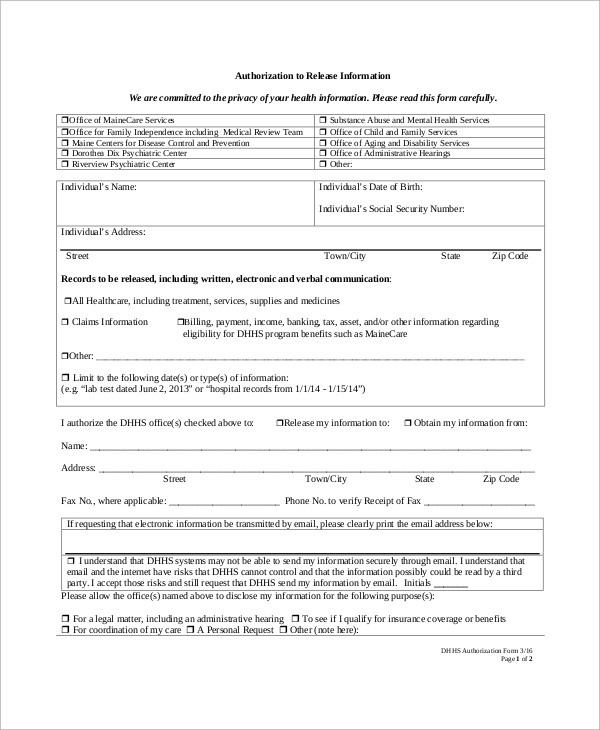
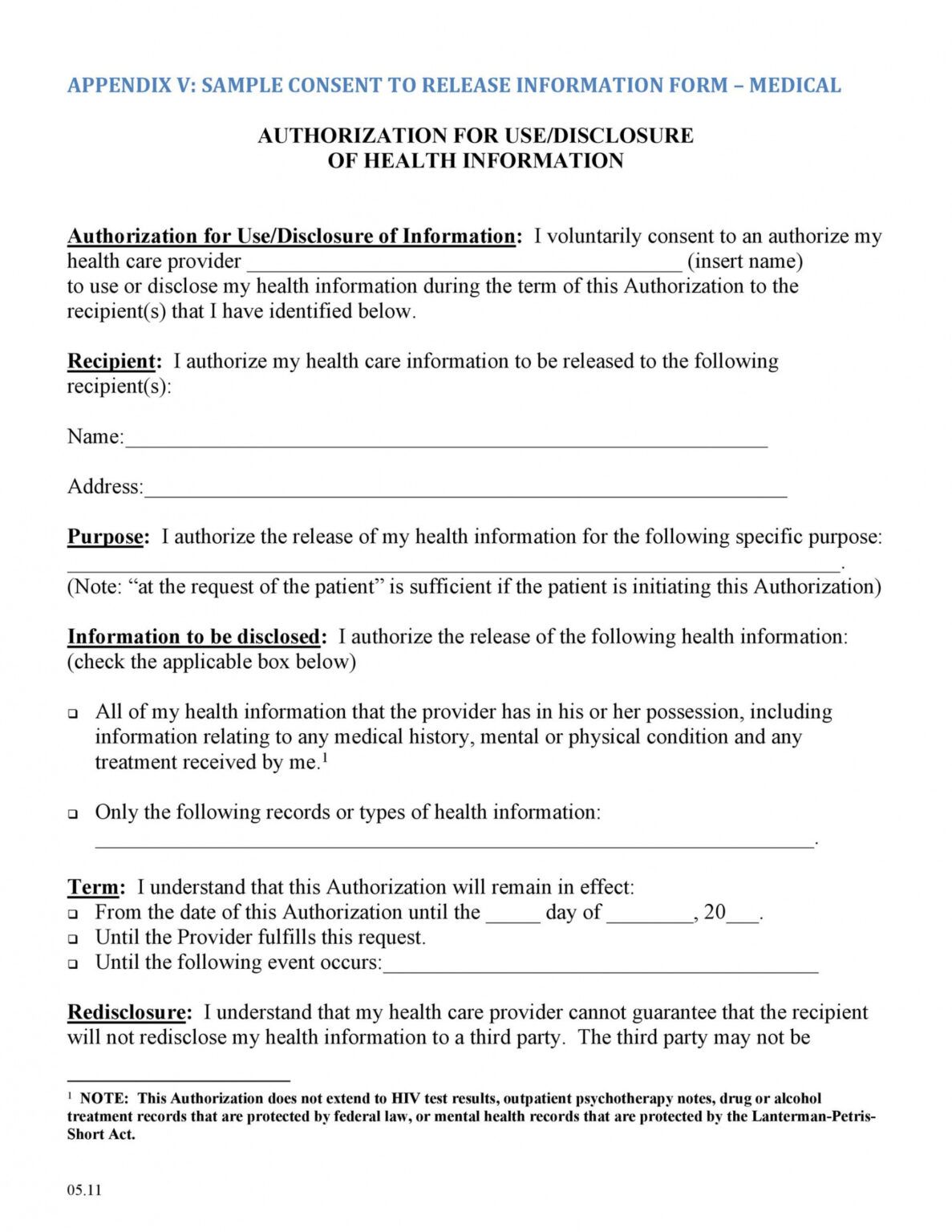
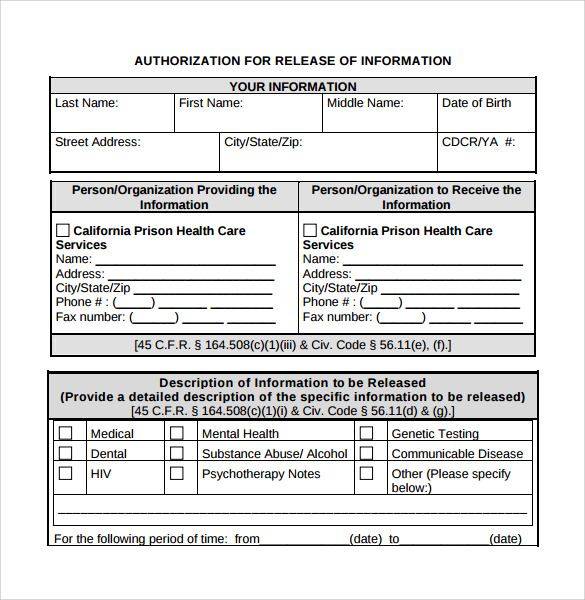
The protected health information to be disclosed includes the following: Web visiting the administrator hub area to locate administrator guidance and release notes. Web section i, print your name or the name of patient whose information is to be released. Web only the information described in this form may be used and/or disclosed as a result of this authorization. Section ii, print the name and address of the facility releasing the information.
Free Release Of Information Form Mental Health Template Doc
Free Mental Health Release Of Information Form
FREE 9+ Sample Release of Information Forms in MS Word PDF
Free Counseling Release Of Information Form Template PDF Example
FREE 9+ Sample Release of Information Forms in MS Word PDF
Release of information form by Becky Peterson Counseling issuu

30 Medical Release Form Templates ᐅ Templatelab Mental Health Release
Therapist Release Of Information Template Fill Online, Printable

Sample Release Of Information Form Mental Health Classles Democracy
FREE 22+ Release of Information Form Samples, PDF, MS Word, Google Docs
Ithenticate and crossref similarity check guidance is now located on a separate site. Web this template for release of information includes all of the information that you need to include and is clean, professional, easy, and fast to use. Web free release of information form template. The form authorizes release of information in accordance with the health insurance portability and accountability act, 45 cfr parts 160 and 164; 5701 and 7332 that you specify. The authorization consenting to release of information form is essential to include in your private practice counseling intake forms. Web collaborate with your colleagues at other practices while meeting your hipaa obligations using our free mental health release of information form. However, hipaa requires ellie mental health to notify me of the potential that information disclosed pursuant to this. ___ assessment information ___ psychiatric evaluation ___ diagnosis ___ results of psychological testing ___ treatment planning notes ___ recommendations Previous treating therapist, current health care providers, parents or school) The protected health information to be disclosed includes the following: To improve the experience for our ithenticate and crossref similiarity check customers we have move their help content onto a separate help site,. Web if you are a legal representative of the person whose information you are requesting, you must provide documentation proving your legal authority to the request this information (for example, power of attorney, healthcare surrogate form, order, appointment of a guardianship, order appointing Web only the information described in this form may be used and/or disclosed as a result of this authorization. Web section i, print your name or the name of patient whose information is to be released.
Web This Form Is Voluntary And Not Required To Receive Services With Valley Behavioral Health Unless The Purpose Of The Treatment Is To Provide Information To The Individual/Entity Identified In This Authorization.
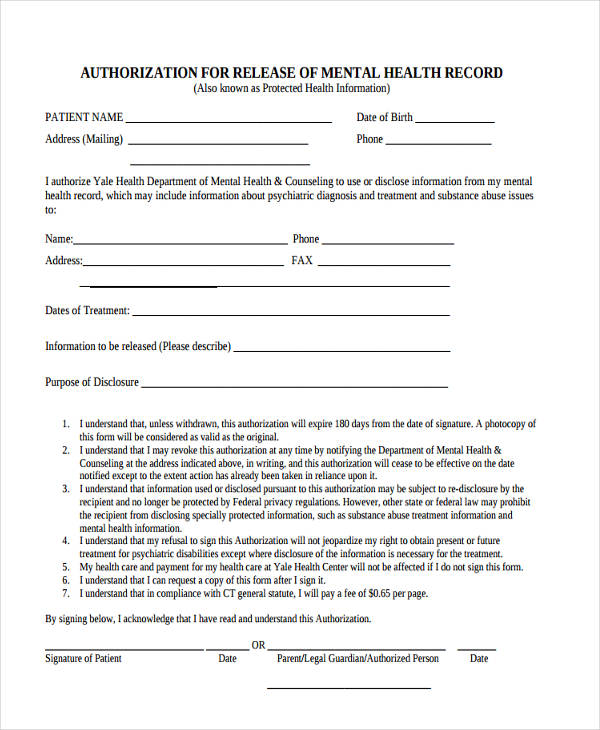
In the past two years, 988 crisis counselors in north carolina have responded to nearly 190,000 calls, texts and chats, providing critical access to mental health and substance use crisis. Web sample standard authorization mental health treatment. Click here to instantly download the free release of information form. Fill in the patient’s information and requestor’s name and contact number.
Web Notice Of Client’s Refusal To Release Information:
I, _______________________________[insert name of patient/client], whose date of birth is ______, authorize [insert name of social work organization] to. Web the information requested on this form is solicited under title 38 u.s.c. To improve the experience for our ithenticate and crossref similiarity check customers we have move their help content onto a separate help site,. 5701 and 7332 that you specify.
Web Press Release — The Nc Department Of Health And Human Services This Week Celebrates The Second Anniversary Of The 988 Suicide And Crisis Lifeline.
Web collaborate with your colleagues at other practices while meeting your hipaa obligations using our free mental health release of information form. This information is confidential and is protected under federal privacy regulations (hipaa) and the nys mental hygiene law and cannot legally be disclosed without my permission. However, hipaa requires ellie mental health to notify me of the potential that information disclosed pursuant to this. Use this form to obtain the required authorization when a request is received for patient information, unless the request received is a facsimile of this form or contains all of the required information.
Section Iii, Provide The Name Of The Person, Facility, And Address That Will Receive The Information.
Fill in the person, provider, or facility that is responsible to release the medical records. Web this template can be used to coordinate the release of confidential information during a client's transition of care or other cicrumstances where private records need to be shared. The authorization consenting to release of information form is essential to include in your private practice counseling intake forms. The protected health information to be disclosed includes the following: